The year opened with renewed political attention on healthcare following the longest federal government shutdown in U.S. history. The stalemate centered on whether to extend enhanced Affordable Care Act tax credits but expanded to broader conversations about the cost of health insurance and alternative ways to pay for care. With the shutdown behind us, will policymakers and the public sustain their focus on issues of healthcare spending and affordability? What other cost-related topics should we watch in the months ahead?
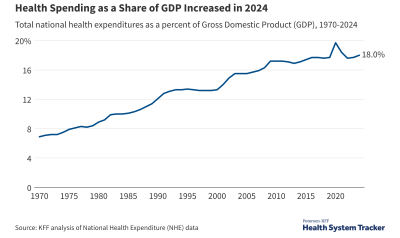
Healthcare represents nearly one in every five dollars spent in the U.S. economy. These costs are shared between the federal government (31%), state and local governments (16%), employers (18%), individuals (6%), and other payers. While federal policymakers have yet to turn to broad cost containment strategies, they continue to explore options for addressing healthcare costs for individuals alongside narrower policies aimed at reducing prices for specific drugs or services.
This brief highlights trends contributing to rising healthcare costs and identifies issues shaping this year’s policy debates, though there is little expectation for much legislative action at the federal level during an election year.
1. Healthcare costs remain top of mind for many Americans
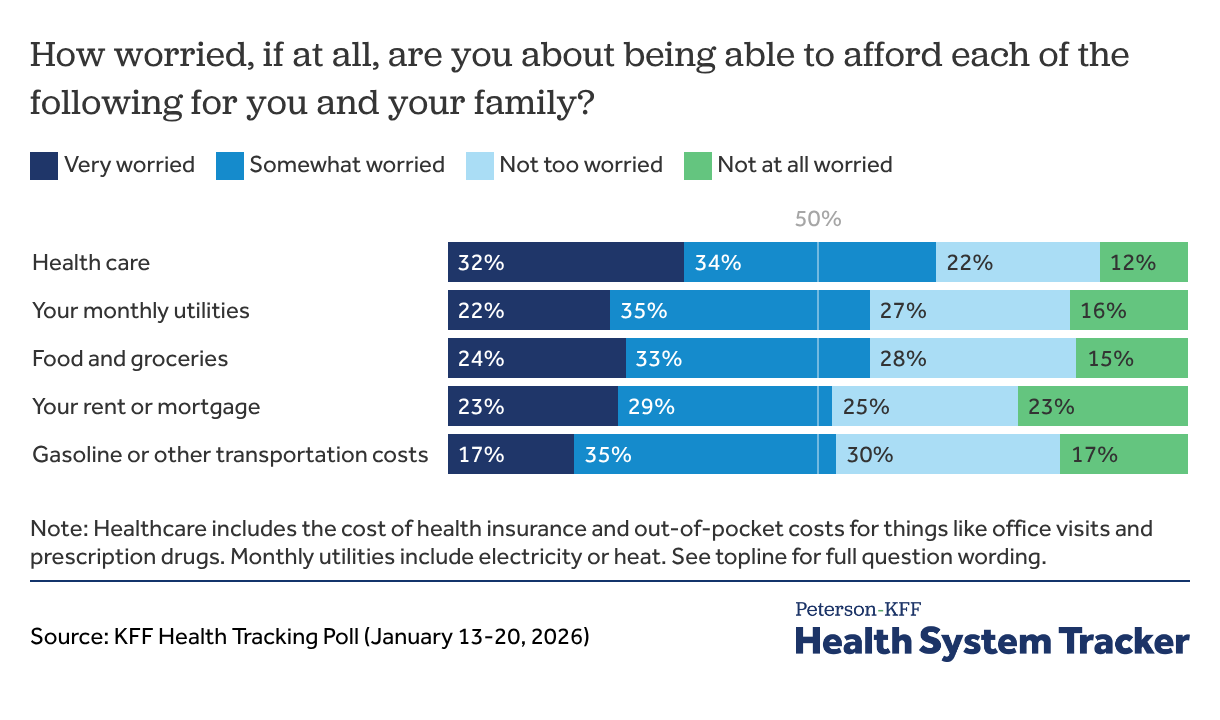
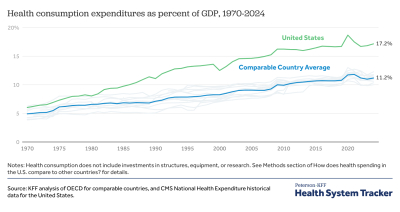
The cost of healthcare in the U.S. continues to grow and remains significantly higher than in peer countries. Recent cost-of-living increases have squeezed household budgets, making healthcare costs the top household expense worrying the public. A family of four with employer-sponsored coverage contributed $6,296 in premiums and incurred $3,564 in out-of-pocket spending in 2023. Private insurance costs are expected to rise even higher in the coming year.
Conversations about affordability will likely be prominent leading up to the midterm elections: Consumers identify healthcare at the center of the affordability crisis, above food, rent, and utilities. Healthcare affordability remains a concern for people with various types of insurance, from individual market plans to employer-sponsored insurance.
2. Premiums have increased across commercial and individual marketplaces
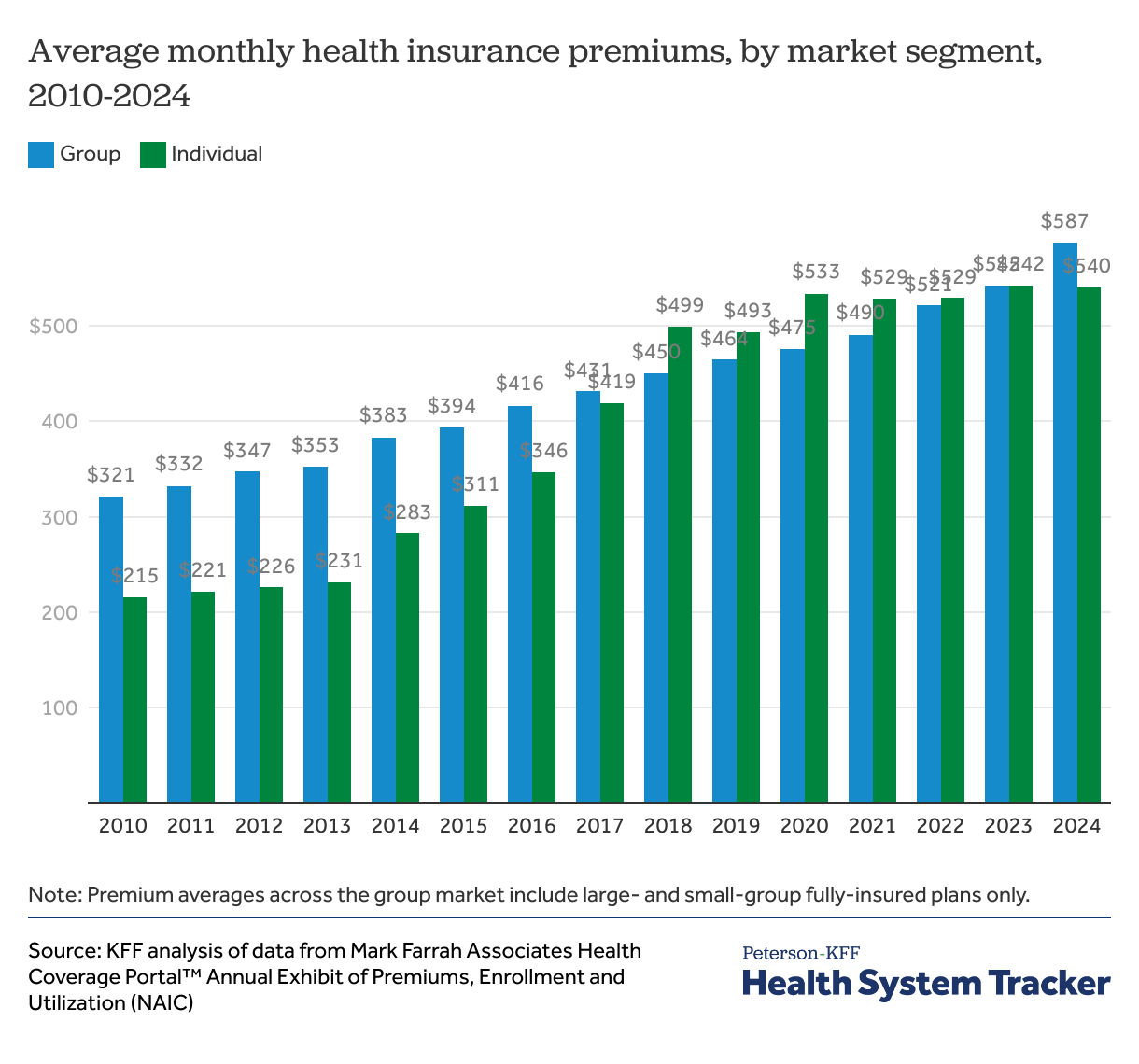
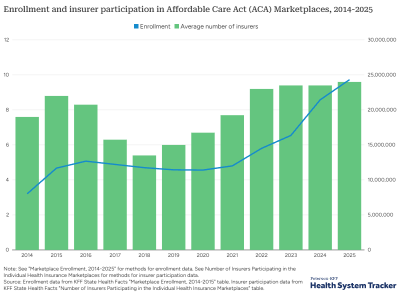
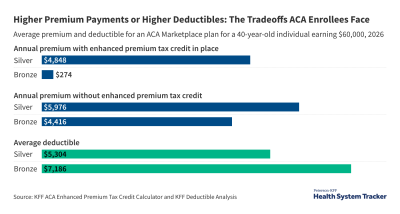
The expiration of the enhanced Affordable Care Act tax credits has led to a significant increase in premium payments for millions of Marketplace enrollees. As Marketplace enrollees face higher monthly premiums, affordability pressures are influencing their enrollment decisions. In 2026, more than 1 million fewer people signed up for a Marketplace plan, though initial numbers may not show the full impact on coverage rates.
In the lead up to the midterm elections, the drivers of healthcare spending and alternative policy proposals—such as restoring enhanced ACA tax credits and reversing Medicaid cuts from Democrats, and ideas like expanding health savings accounts from Republicans—may attract sustained attention.
3. The public and private sectors are looking for solutions as U.S. spending on prescription drugs continues to increase
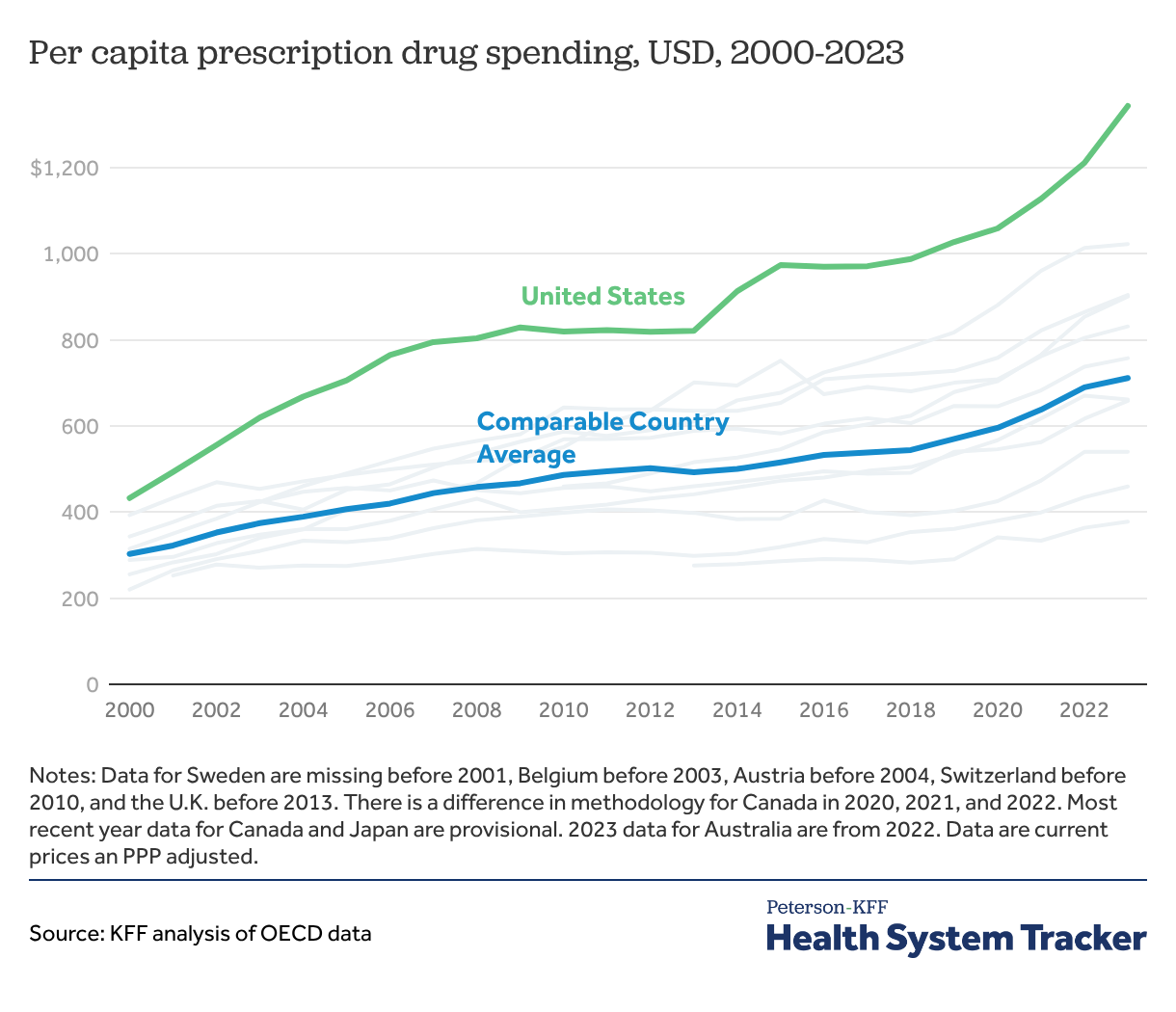
The U.S. spends roughly twice as much per capita on prescription drugs compared to peer nations, and many Americans identify drug costs as an important political issue and an affordability concern. The Inflation Reduction Act, including Medicare price negotiations for a list of eligible drugs, led to lower costs for some beneficiaries and the federal government. However, the U.S. continues to pay more for the same drugs than peer nations.
The Trump Administration unveiled a series of initiatives aimed at addressing prescription drug affordability, including the launch of the TrumpRx website, which seeks to negotiate “most favored nation” individual cash-price deals directly with pharmaceutical companies. Because most Americans obtain their medications through insurance coverage, the breadth of the impact of these deals, which are aimed at decreasing the cash price of prescription drugs, may be modest. Some insurers, increased their 2026 premiums with the expectation of higher drug costs due to the threat of tariffs from the White House.
Congress and President Trump have also signaled an interest in reforming prescription benefit managers (PBMs). The Consolidated Appropriations Act of 2026 was signed into law in February and introduced reporting requirements and structural changes for PBM payments. This includes moving compensation to a service-based flat-fee instead of percentage based in Medicare and mandating that any drug rebates be fully passed through to the plan sponsor for Medicare and group health plans. Other recent federal actions have sought to continue to reduce drug prices through PBM reform.
Employers are deciding if and how they should cover the popular GLP-1 agonists used to treat diabetes, weight loss, and other conditions. The cost burden led some employers to drop coverage for weight loss in 2026, though costs may be mitigated by a growing direct-to-consumer market, new oral pills that are easier to administer and potentially less costly, and virtual solutions to manage costs and maximize outcomes.
Further, many high-cost drugs (e.g., cell and gene therapies) are administered in high-cost settings, such as hospital outpatient departments, contributing to hospitals accounting for 40% of overall healthcare spending growth in the past year.
Related Content:

4. Price transparency for healthcare prices has momentum
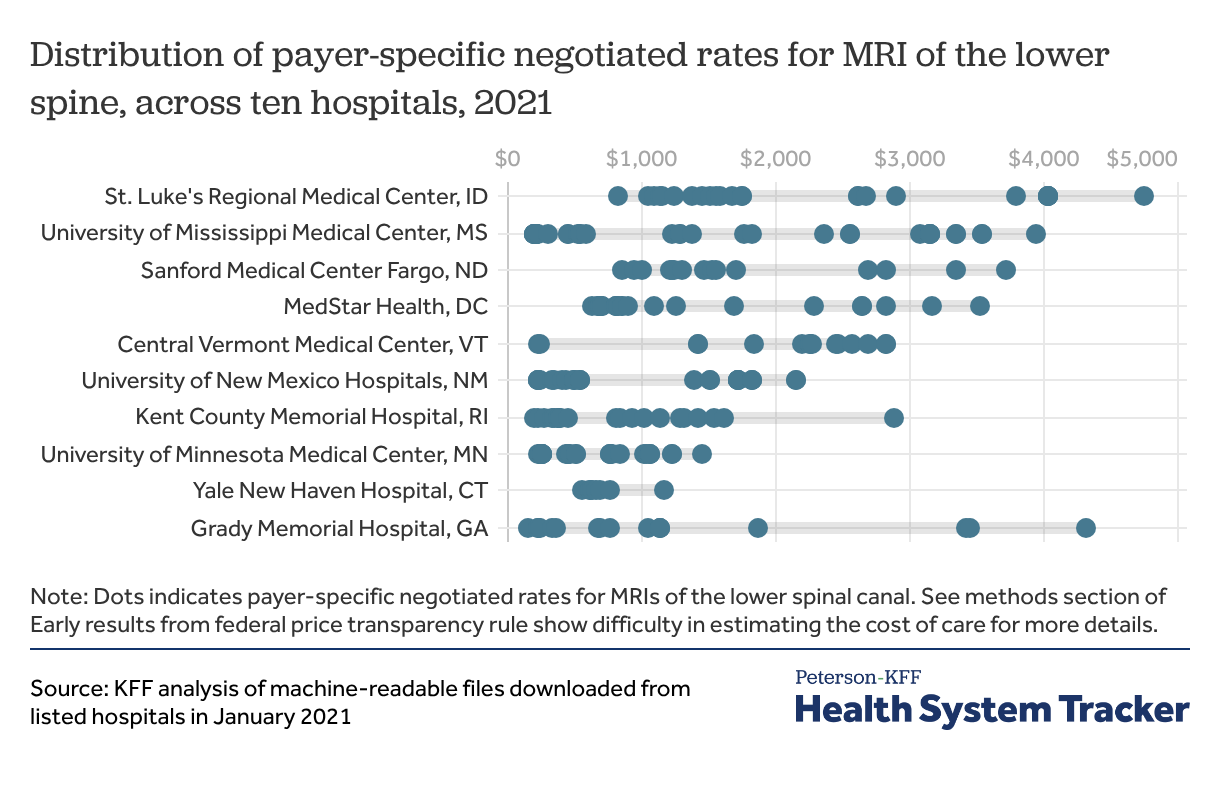
Price transparency data shows that prices for the same service can vary depending on the payer and across providers. Providing clear and accurate pricing should, in theory, improve the ability of consumers and employers to negotiate or shop for lower prices. Many employers, consumers, and advocates believe this data could improve affordability by allowing more informed purchasing choices. In January, the CEOs of five major commercial health insurers to Congress that they support improving price transparency. For self-insured employers, this may enable contracting with lower-priced provider networks. Employees and employers may find lower-priced services. Insurance companies have also used the data to negotiate better prices.
Regulations released during the first Trump administration required both hospitals and health plans to release pricing information, yet researchers and consumers have found it difficult to make use of current data, limiting its impact. The current administration and Congress have recently proposed policies and updated regulations to further price transparency. President Trump’s recently released healthcare plan includes a requirement for any healthcare provider or insurer who accepts Medicare or Medicaid to post their pricing and fees in their place of business, and HHS Secretary Kennedy recently announced that the federal government will host a hospital service price list. The Patients Deserve Price Tags Act, which would codify existing transparency rules and expand disclosure requirements, has bipartisan support in both the House and Senate. While previous legislation stalled after passing the House, a focus on healthcare costs could spur discussion before the midterm elections.
Related Content:
Related Content:
5. Federal and state policymakers show interest in addressing the impacts of healthcare consolidation
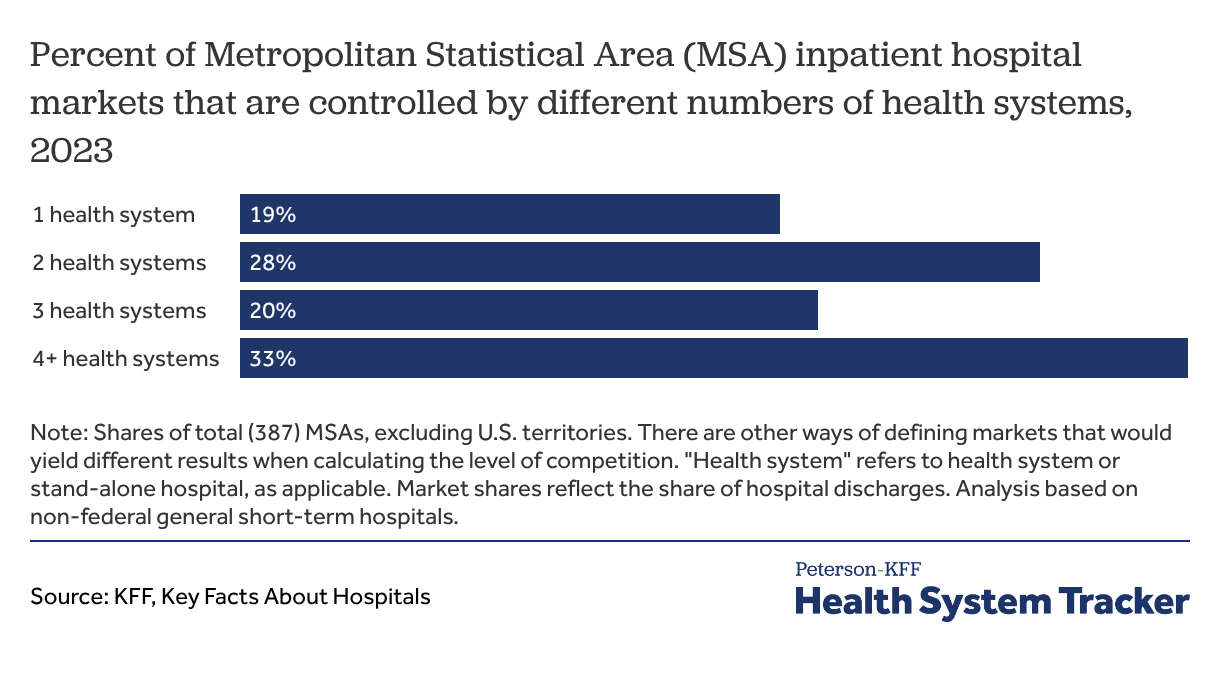
Although mergers and other types of healthcare provider consolidation are promoted as, among other things, improving continuity of care and reducing administrative overhead, they also reduce competition. Provider markets have become highly consolidated. According to KFF analysis, in 2023, one or two health systems provided all inpatient commercial hospital care in about half of U.S. metropolitan areas. A large body of evidence has found that provider consolidation contributes to higher prices, with unclear effects on quality. Consolidation between insurers and providers, as well as insurer market competition, has also received scrutiny, though there is less evidence about its impact.
In addition to recent price transparency momentum, policymakers at both the federal and state level see opportunities to reduce consolidation or increase the competitiveness of healthcare markets in other ways. For example, recent bipartisan legislative proposals include restrictions on anti-competitive contract clauses between providers and payers and prohibitions on some types of vertical consolidation, such as owning both an insurance company and a healthcare provider.
6. The use of artificial intelligence in healthcare is likely to accelerate coding intensity, placing upward pressure on healthcare spending
Artificial intelligence (AI) is rapidly reshaping the U.S. healthcare system, notably through the proliferation of ambient scribes. For healthcare providers, these new tools offer the promise of reducing administrative burden and burnout by making it easier to document patient visits. It is estimated that ambient scribes are now used by 10% or more of U.S. physicians.
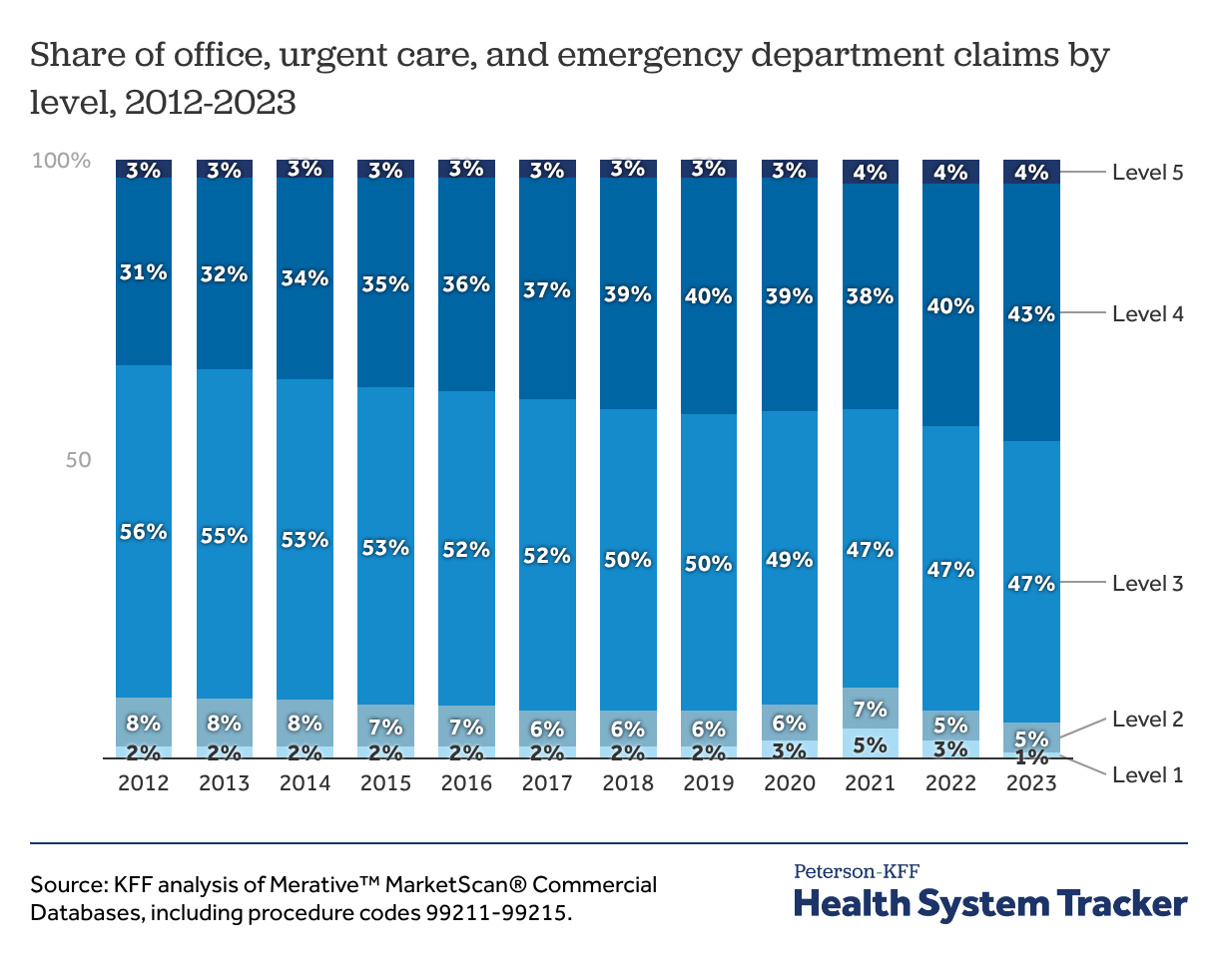
For healthcare organizations, AI documentation and coding tools automate how a patient visit is captured and translated into medical claims submissions. AI-enabled tools can now thoroughly document patient visits. Better documentation increases the proportion of visits that can be coded as higher complexity, which in turn increases billing. While the proportion of higher-complexity office visits has been growing steadily over the past decade, in part due to an aging, more complex patient population, AI documentation and coding tools will likely accelerate this trend. Payers are already finding that AI-driven documentation and coding is increasing billing amounts (irrespective of the health of the underlying patient population or changes to care delivery). In response, payers are deploying their own changes to coding, utilization management, and payment policies to combat rising spending.
7. States are responding to funding and program implementation pressures with changes to Medicaid beginning in 2027
CBO estimates that the 2025 budget reconciliation bill (also known as the One Big Beautiful Bill Act, or OBBBA) will reduce federal spending in Medicaid by over $900 billion over a decade. The OBBBA requires states to implement community engagement requirements for the population of Medicaid enrollees who were made eligible for the program through the Affordable Care Act’s Medicaid expansion. Starting in 2027, about 20 million people will be required to verify that they have worked 80 hours per month, completed other qualified activities, or qualify for an exemption from the requirements. The OBBBA also reduces federal Medicaid spending through financing changes. The law prevents states from establishing new provider taxes or increasing existing taxes and phases down certain existing taxes in Medicaid expansion states. It also caps state-directed payments for hospital and nursing facility services at 100% of Medicare rates for expansion states and at 110% of Medicare rates for non-expansion states. These financing changes could result in reduced payments to providers.
Medicaid changes are expected to create budgetary challenges for states, providers, and beneficiaries. States are grappling with shouldering more costs of the Medicaid program as well as implementation costs of the new community engagement requirements and more frequent eligibility redeterminations. In response to anticipated budget shortfalls, states are weighing a variety of actions to cut Medicaid reimbursement rates and limit benefits like dental care. Providers expect to face revenue reductions and rising costs from uncompensated care. CBO also estimates that about 10 million people will become uninsured as a result of the healthcare provisions in OBBBA.
8. Effective distribution of the Rural Health Transformation Funds will require rapid state action
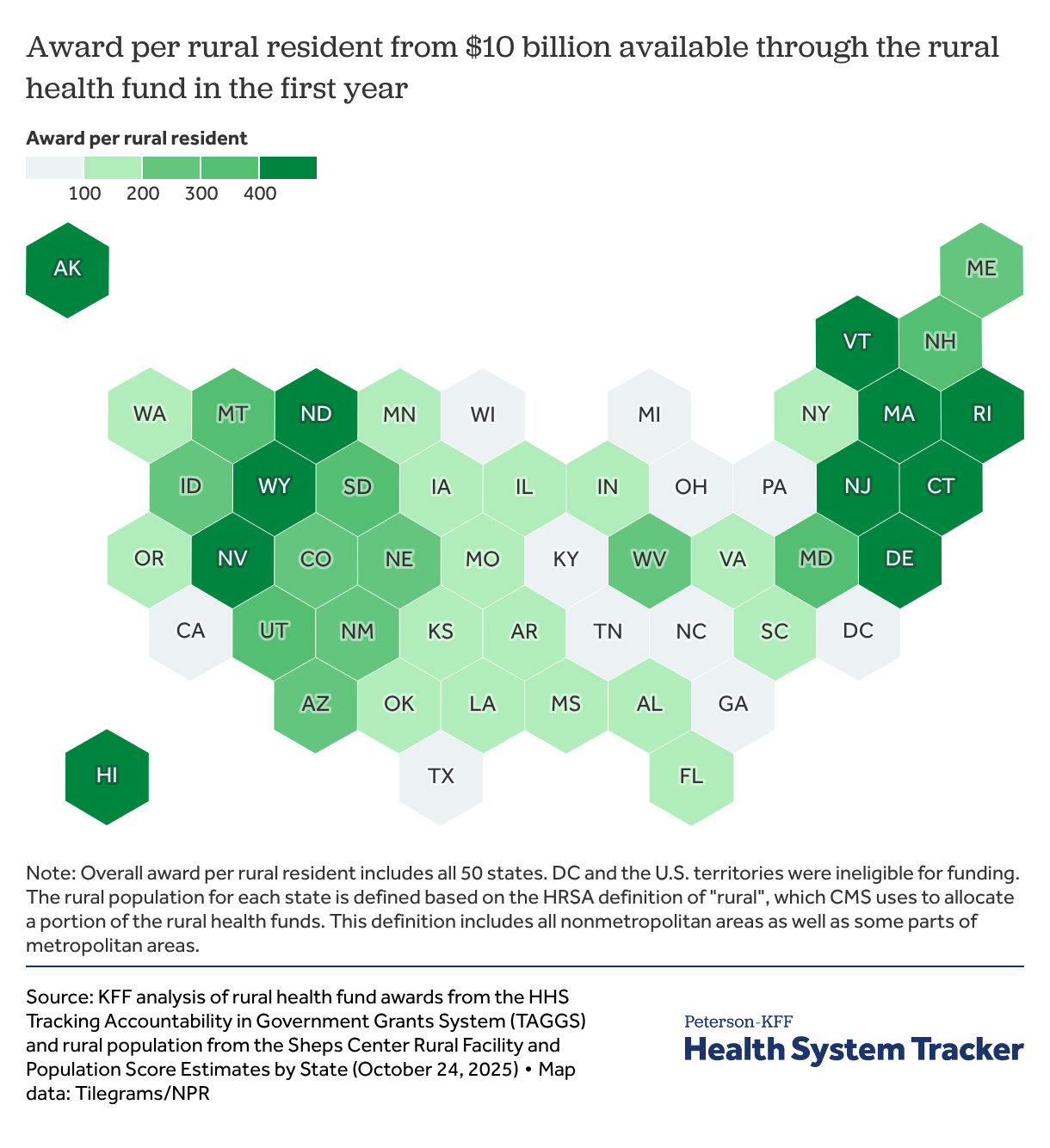
State officials are working to implement the Rural Health Transformation program established by OBBBA, which makes available $50 billion to states over five years. Awarded grants for 2026 total $10 billion and range between $147 million and $281 million per state. Half of the funds will be evenly divided between the states and half will be allocated by CMS based on a variety of factors, including the share of the state population living in a rural area, proportion of rural health facilities, and CMS discretion as outlined in the Notice of Funding Opportunity. States must move quickly to effectively plan for and spend the money. Rural Health Transformation funds were added to the 2025 reconciliation law to address lawmaker concerns of the potential effects of cuts to Medicaid funding on rural areas, though the funds will not fully offset the impact of the Medicaid funding cuts in rural areas. The Medicaid cuts are permanent and exceed the new temporary rural health funding in rural communities and payments to providers for care cannot exceed 15% of total transformation fund award.
Each state has proposed using some of the funds to deploy various technology-enabled healthcare solutions, including expanding telehealth infrastructure, deploying remote patient monitoring for certain conditions and patient populations, modernizing electronic health record systems, or using AI to support administrative functions, clinical decision-making, and patient management of care. States have also proposed spending the money on a wide variety of other initiatives, including alternative payment models or care delivery in lower-cost settings such as mobile clinics or via telehealth.
In addition to committing funds, states have adopted, or agreed to adopt, policies that may make them eligible for additional funds. For example, to support the clinical workforce, some states committed to participating in interstate licensure compacts and expanding scope of practice for professions such as pharmacists, paramedics, and dental hygienists. Additionally, almost half of states made policy commitments to implement SNAP restrictions on certain foods and require providers to complete continuing medical education activities on nutrition to align with Trump administration’s focus on addressing the drivers of childhood chronic disease.
Note: Lynne Cotter, Emma Wager, and Matthew Rae are with KFF. Hattie Xu, Tom Lebert, Julia Harris, and Brad Brockbank are with the Peterson Center on Healthcare.
Related Content:
The Peterson Center on Healthcare and KFF are partnering to monitor how well the U.S. healthcare system is performing in terms of quality and cost.