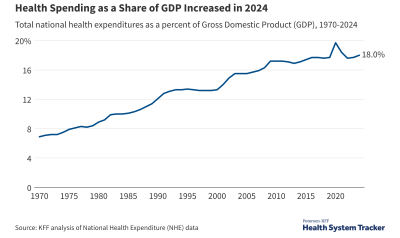
The recent slowdown in health spending growth continued through 2013, according to a new report released by the Centers for Medicare and Medicaid Services (CMS). Health spending per capita grew at 2.9% in 2013, a continuation of the historically low annual growth rates in recent years. In total, the U.S. spent $2.9 trillion on healthcare and related expenses in 2013. As health spending grew at a similar rate as the overall economy, the health sector continues to represent 17.4% of the nation’s economy. (Health spending as a percent of gross domestic product has remained flat at this level since 2009.)
U.S. health care spending per capita has risen at historically low rates in recent years
Health care spending per person in the U.S. has risen at historically low levels during the last few years, raising the question as to how much of the slowdown can be attributed to the severe recession and slow economic recovery and how much may be the result of structural changes in the health system (such as higher deductibles and changes in provider reimbursement policies). This is important because it helps tell us if and by how much health spending will increase as the economy recovers. The federal government projects health spending per capita will grow more quickly over the next decade as the economy gradually recovers and as more people gain coverage under the Affordable Care Act.
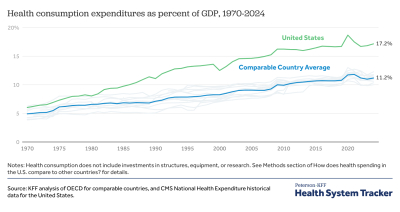
Health spending growth has slowed in the U.S. and in comparable countries
The recent slowdown in per person health spending occurred in the U.S. as well as in comparable countries, suggesting that the global recession played a meaningful part in the reduction. However, slower growth in new medical technologies could also explain a global slowdown.
Low growth rates have persisted for five years, sparking researchers to look for the causes
Researchers have taken a variety of approaches to explain why health spending growth has fallen to and persisted at such low levels. Analyses by Dranove and colleagues and the Kaiser Family Foundation and the Altarum Institute conclude that economic factors explain most of the recent slowdown. Holohan and McMorrow show that health care spending growth started to fall prior to the recession and conclude that the longer period of decline was a response to falling real incomes and shifts in coverage away from more generous employer-sponsored coverage to public plans that pay providers less and to uninsurance.
Cutler and Sahni conclude that the most recent recession explained only 37% of the slowdown during the period, and suggest that a sizeable portion of the spending slowdown is due to structural changes in the health system. Chandra and colleagues show that real (adjusted for inflation) health care spending growth rates fell rapidly after 2002 and suggest three factors as responsible for the decline: the rapid diffusion of high-deductible health plans combined with the decline in the percentage of people with insurance; cuts in Medicaid benefits and reimbursement rates caused by state budgets constraints; and a slowdown in the diffusion of new technologies.
Related Content:
What types of structural changes in the health care system may be contributing to the slowdown
There is consensus that while the economy has played a role in the slowdown, changes in the health system are also an important factor. Structural changes that have occurred during the last decade include higher cost sharing in private health insurance (which discourages the use of health care services), the loss of employer-based coverage (with people moving to lower-paying coverage or no coverage), lowering of payments to providers in public programs (lower prices reduce growth), less use of expensive technologies, and providers producing care for less cost (spurred on by decreased reimbursement or payment changes such as reduced payments for readmissions).
While all of these measures reduce costs below previous levels, they may not lead to further reductions in cost growth. For example, raising cost sharing will reduce the number of services enrollees are expected to use and lower the growth rate for the following year, but to keep lowering the growth rate cost sharing must continue to increase, which may not be practical after a certain point. The difference between one-time cost reductions and the approaches that lower growth rates over time is discussed here.
Medicare spending slowed for different reasons than private spending
A Congressional Budget Office (CBO) analysis found that the economic downturn did not have the same effect on Medicare spending that it appears to have had on overall health spending. Rather, structural changes, including reductions in provider payment from the Affordable Care Act and sequestration under the Budget Control Act of 2011, may have helped to moderate Medicare spending growth. Compared to 2010 projections, Medicare spending is now expected to be about $1,200 lower per beneficiary in 2014 and about $2,400 lower in 2019.
An annual percentage point difference in growth rates makes a very large difference in spending over time
What may seem to be small differences in growth rates are very meaningful over time. Per capita expenditures are projected to grow from $9,695 in 2014 to $15,618 in 2024, which is an average annual growth rate of about 5 percent. If growth rates were 1 percentage point lower each year over that same period, per capita spending would fall be $1,555 lower than expected, which would be a decrease in total expected spending by about $500 billion in 2024 alone and about $2.3 trillion in the 10-year period (2015-2024). If growth rates were 1 percentage point higher each year, per capita spending would rise to $17,173 in 2024, which would increase total health spending by over $500 billion in 2024 alone and by about $2.5 trillion in the 10-year period.
The Peterson Center on Healthcare and KFF are partnering to monitor how well the U.S. healthcare system is performing in terms of quality and cost.