The COVID-19 pandemic has dramatically affected the utilization of health services in the United States. In the early months of the pandemic, there was an abrupt and sizable decrease in spending on health services. However, a notable exception has been in the use of telehealth services, which has increased substantially during this time. In April 2020, one analysis found that 13% of health care claim lines were for telehealth services, up from 0.15% in April 2019. As discussed more in this brief, mental health services have accounted for a large share of telehealth visits, with multiple insurers reporting that over a third of telehealth visits were for mental health.
To encourage social distancing and improve access to care during the pandemic, the federal government has issued guidance to private insurance plans encouraging the use of telehealth during the pandemic. Similarly, Medicare has waived co-payments for beneficiaries and now pays providers the same rate for a telehealth visit as an office visit. In addition, since the start of the pandemic, many state governments have implemented new policies regarding telehealth usage in their Medicaid programs.
With these developments in mind, we reviewed a summary of private insurers’ responses to the pandemic, put together by America’s Health Insurance Plans (AHIP). We systematically collected data from this summary and merged it onto enrollment data to better understand how private health insurers are responding to the COVID-19 pandemic. We specifically focus on four policies or actions that promote telehealth usage: waiving cost-sharing for select telehealth services, offering or expanding telehealth access to mental health and/or substance use services, and instituting provider payment parity for telehealth. Using data from Mark Farrah Associates TM, we estimate how many individual market and fully-insured group market enrollees are in plans with these new telehealth policies. While some plans offered similar policies and benefits before the pandemic (e.g. coverage of mental health or substance use telehealth visits), these data reflect enrollees that are newly affected as a result of COVID-driven policy changes by insurers. Our estimates do not include the substantial portion (61%) of the group market enrolled in self-insured plans through their employers, because the benefit designs of these plans generally are left to the discretion of the employer.
Findings
Waived cost-sharing. Over 30 million people are enrolled in individual market and fully-insured group plans that waived cost-sharing for all telehealth services (beyond COVID-19 testing and treatment) at some point during the pandemic.[1] 38% of individual market enrollees are in a plan that has recently waived cost-sharing for non-COVID telehealth services, including 7% who live in states that currently mandate it and 31% who are enrolled in plans outside those states that did so voluntarily. Similarly, 52% of enrollees in the fully-insured group market are in a plan that has waived cost-sharing for telehealth services, 11% of whom live in a state that has currently mandated it and 41% in plans outside those states that did so voluntarily.
Private insurance plans have taken a variety of steps to expand telemedicine uptake and access during the pandemic
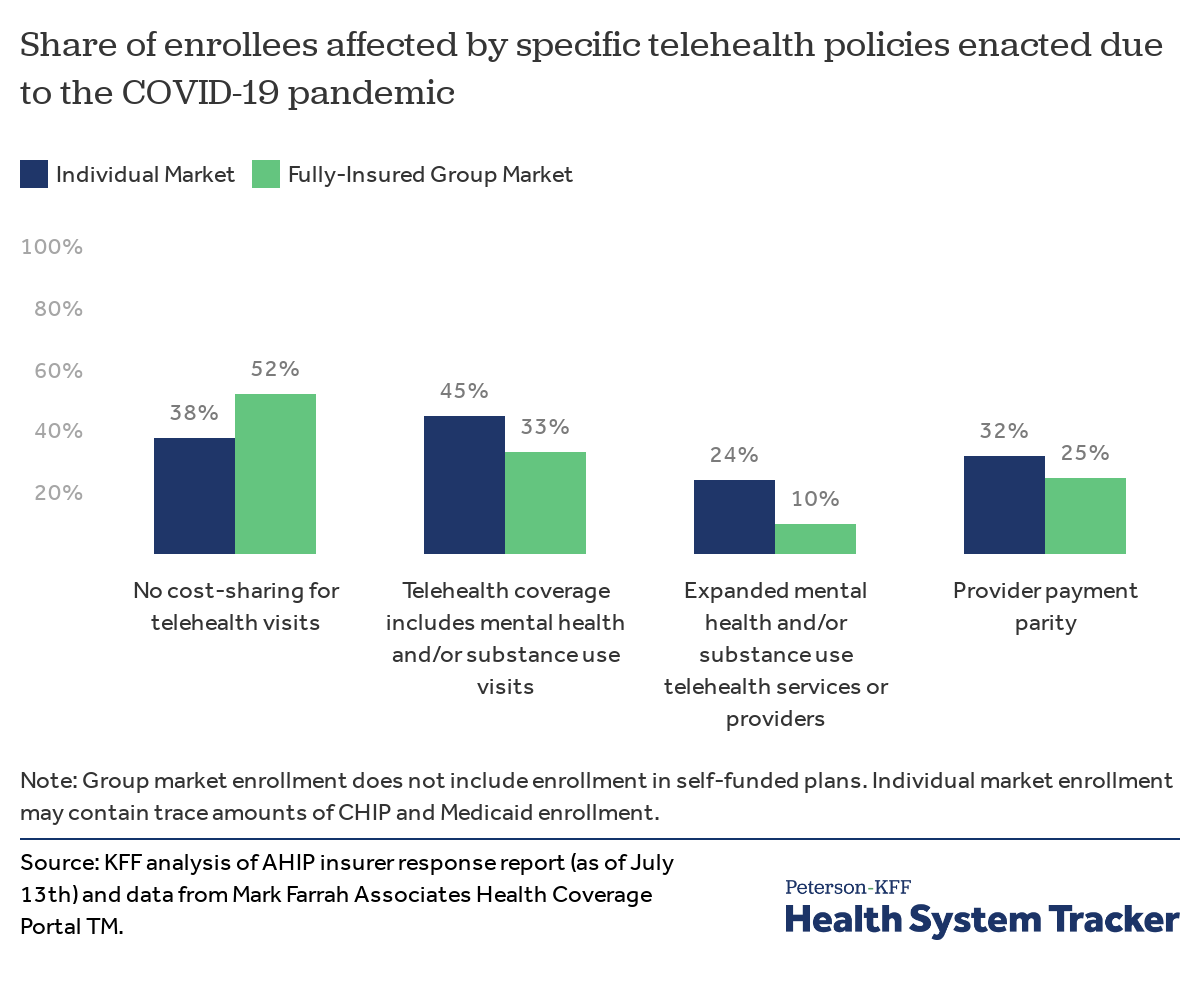
Telehealth coverage includes mental health and/or substance use visits. At least 30 health plans have started including mental health and/or substance use visits in their allowable telehealth services since the start of the pandemic. Combined, these plans cover 45% of enrollees in the individual market and 33% in the fully-insured group market.
Related Content:
Expanded mental health and/or substance use telehealth services or providers. AHIP identifies 15 health plans that expanded access to mental health and/or substance use via telehealth at some point during the pandemic, including adding new providers or contracting with companies that offer counseling services via telehealth. These plans cover 24% of enrollees in the individual market and 10% in the group market. For example, Blue Cross and Blue Shield of Massachusetts reported that almost half of their telehealth visits since the pandemic began have been for mental health services. To meet the demand, they added more than 400 mental health clinicians to its network since March 1, increasing the number of mental health clinicians to nearly 15,000.
Telehealth provider payment parity. More than 17 million enrollees are in private plans that are paying providers the same rate for telehealth visits as office visits, often referred to as provider payment parity. About a third (32%) of individual market enrollees are in a plan with telehealth provider payment parity, including 27% who live in states that currently mandate it and 5% who are enrolled in plans outside those states that did so voluntarily. Similarly, a quarter (25%) of enrollees in the fully-insured group market are in a plan that has instituted telehealth provider parity, 22% of whom live in a state that has currently mandated it and 3% in plans outside those states that did so voluntarily. Payment parity between telehealth and office visits can expand access and capacity, but it also assists providers who lost significant revenue with the stay-at-home orders and accompanying deferral of many health services.
Discussion
Proponents of telehealth have long-advocated that the increased use of telehealth services can improve access and outcomes for patients, decrease costs, and facilitate the sharing of information between healthcare professionals. However, many barriers have impeded the expansion of telehealth services in the U.S., including the highly regulated and fragmented healthcare system, technology challenges, reimbursement issues, and provider resistance.
Although most employer plans covered telemedicine services before the pandemic, use of these services had been quite low. While the increase in telehealth has not offset the drop in in-person visits, the pandemic has created significant policy changes that overcame existing barriers and could potentially lead to a lasting uptake in telehealth. Overall, it is unclear whether we will continue to see high rates of telehealth utilization once the pandemic is over. Many of the policies enacted for private insurance plans have sunset dates, though several have extended the policies, some through the end of 2020 or until the public emergency is over.
If telemedicine use continues to pick up as a result of the pandemic, this could have implications for health spending and outcomes. On one hand, if providers are reimbursed at lower rates, telehealth could offer savings. On the other hand, there may be concerns that these services could be additive (increasing health utilization overall) rather than just replacing in-person visits. Another important question for researchers and policymakers to continue monitoring is whether telehealth services are providing care that can truly replace in-person visits.
Methods
We reviewed a summary of private insurers responses to the pandemic, put together by America’s Health Insurance Plans (AHIP), the trade association representing private insurers. We systematically collected data from this summary as of July 13. For plans included in the AHIP summary, we merged on enrollment data as of the first quarter of 2020. Enrollment data were reported to the National Association of Insurance Commissioners (NAIC) and compiled by Mark Farrah Associated TM. State actions on telehealth policies were sourced from KFF’s tracker of State Data and Policy Actions to Address Coronavirus, which is updated daily.
[1] There are many more people enrolled in self-funded plans that may have also received these benefits, but we do not include them in this analysis as the decision generally is left to the employer and there is no systematic collection of data on employer decisions.
The Peterson Center on Healthcare and KFF are partnering to monitor how well the U.S. healthcare system is performing in terms of quality and cost.