There has been considerable attention to the issue of “surprise-medical bills,” or the occurrence of out-of-network charges when a patient was unaware of charges and therefore could not reasonably avoid them. Earlier this year, we estimated that 18% of emergency visits and 16% of inpatient admissions at in-network hospitals resulted in at least one out-of-network bill. Out-of-network charges typically leave patients exposed to higher costs, both through plan cost-sharing requirements as well as “balance billing” from the provider. Balance billing is a practice in which out-of-network providers – who have not negotiated discounted rates with an insurer – charge patients the difference between what they received from the insurer and their full charge for a service. For an in-depth explanation of out-of-network billing, consumer protections and current legislative proposals, see our earlier brief: An examination of surprise medical bills and proposals to protect consumers from them.
This analysis looks at the prevalence of potential surprise medical bills based on patient diagnosis, emergency visits, and type of inpatient admission. We find that these factors can also affect the likelihood that patients may incur surprise out-of-network bills. As in our earlier brief, we analyzed insurance claims from large employer plans to identify how often inpatient admissions, emergency room visits or outpatient surgeries result in a claim from an out-of-network provider.
Patients with surgical and mental health admissions may be at higher risk of surprise medical bills
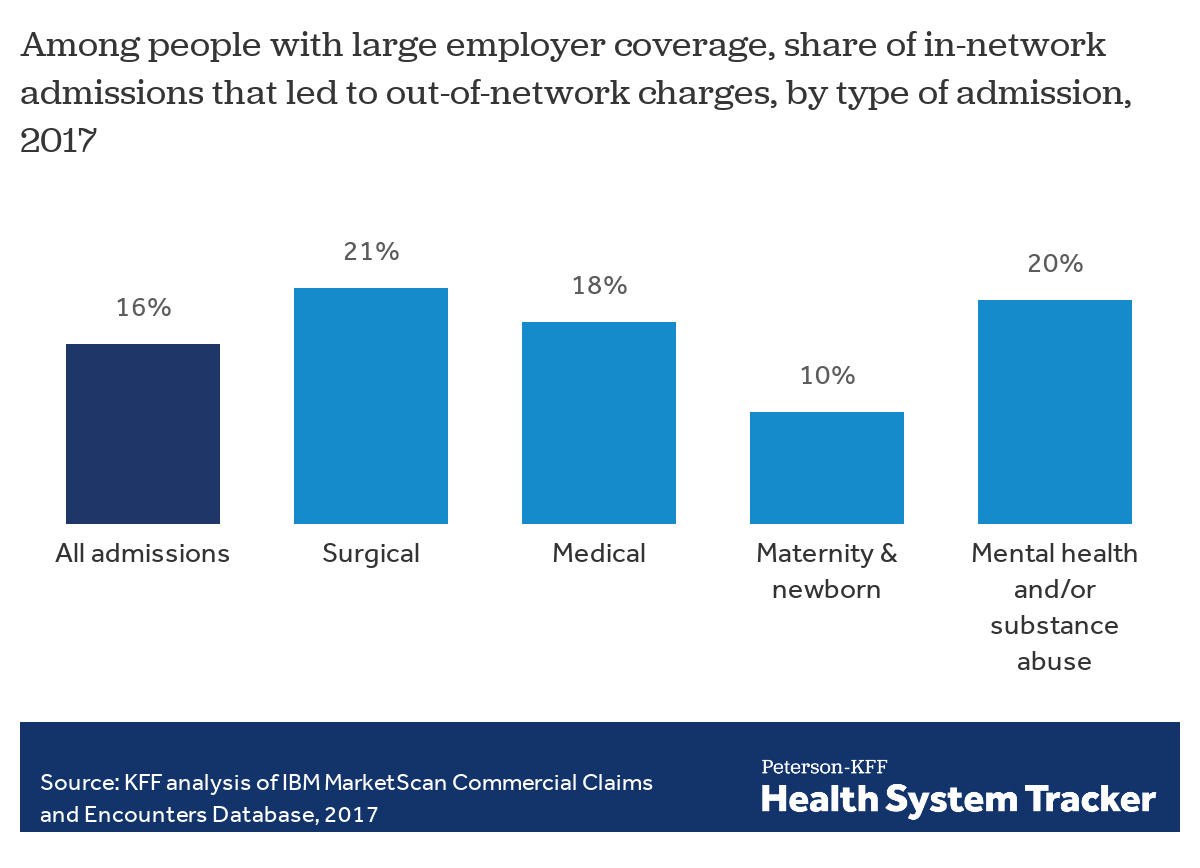
Overall, 16% of admissions at an in-network hospital lead to at least one out-of-network charge. Compared to all admissions, admissions for surgery are more likely to lead to an out-of-network charge (21%). One in five in-network admissions for mental health and/or substance abuse (20%) also lead to out-of-network charges, while admissions for childbirth and newborn care are less likely to include a claim from an out-of-network provider (10%).
Heart attack patients may be more at risk of surprise medical bills
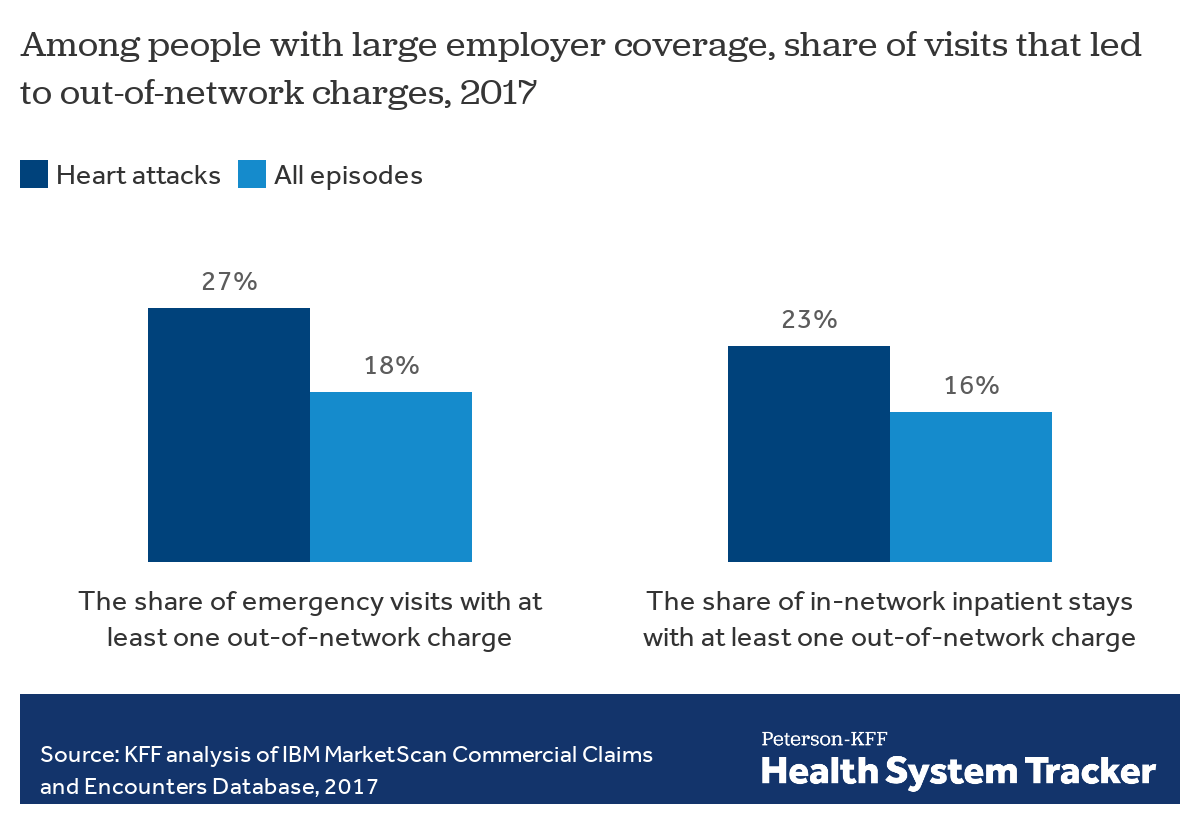
We examined the incidence of out-of-network charges among people covered by large employer health plans who received emergency services or inpatient stays at in-network facilities for a heart attack. The incidence of out-of-network charges was 50% higher for heart attacks compared to the incidence rate of all diagnoses for both emergency services (27% vs. 18%) and for inpatient admission at in-network facilities (23% vs. 16%), respectively.
We also examined the incidence of out-of-network charges among patients having breast cancer surgery. Our method of identifying potential surprise medical bills generally counts out-of-network charges incurred on the same day as a patient’s emergency room visit and charges incurred during the same days that a patient was treated at in-network inpatient facility. This method, however, may not capture all of the surprise bills that certain patients may face. In particular, patients undergoing a mastectomy or lumpectomy — procedures typically performed on an outpatient basis to treat breast cancer — also receive surgical pathology services to diagnose and stage the cancer and determine appropriate treatment. These surgical pathology services may be provided on the same day or on a different day than the breast cancer surgery.
Read more from
Surprise BIlls
See more briefs and data.
Women undergoing mastectomies may have a higher risk of surprise medical bills
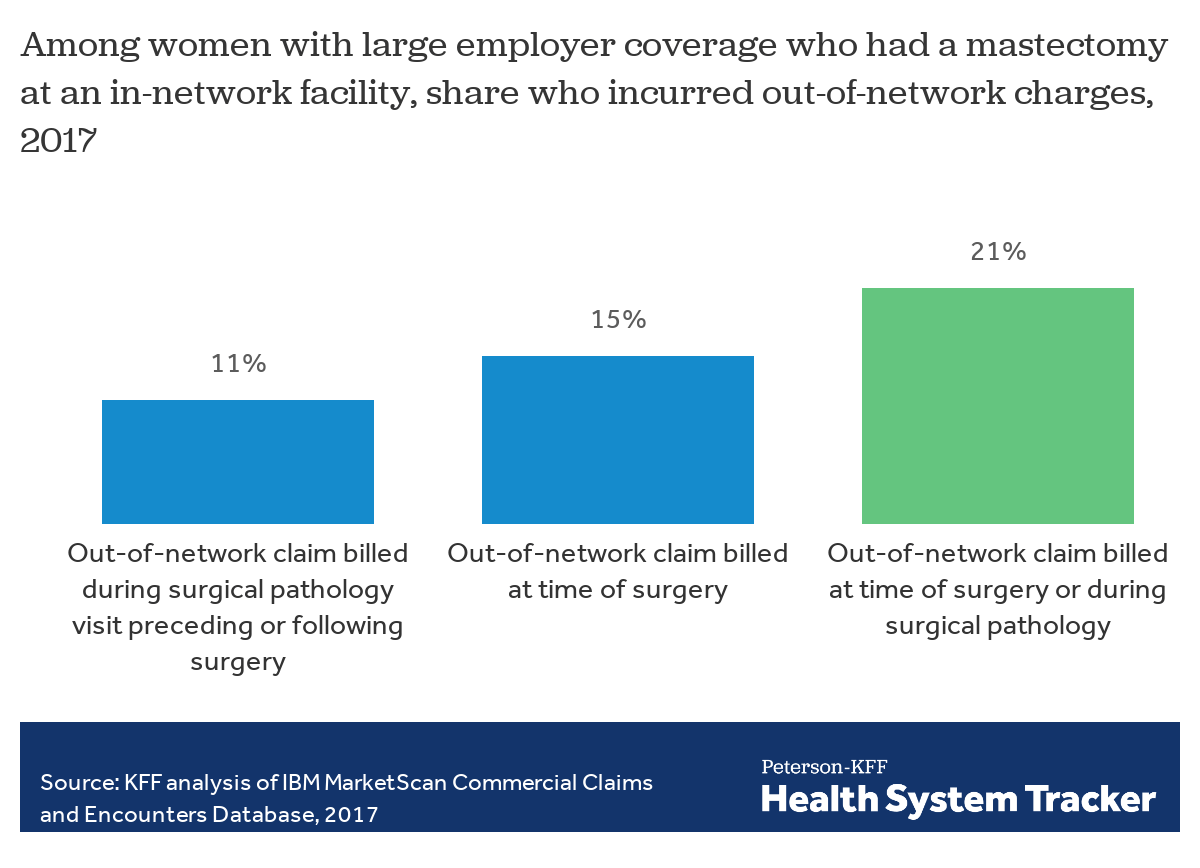
To account for the break in time between the date of surgery and when the surgical pathology is performed, we analyzed claims of women covered by large employer plans who had a mastectomy at in-network facilities (either inpatient hospitals or outpatient surgical facilities) who also received out-of-network provider claims on the day of the surgery or out-of-network surgical pathology services performed on a different date. We found that 21% of women undergoing mastectomies experienced out-of-network provider charges, including surgical pathology charges; for 15% of women, the out-of-network charges were billed on the day or during the inpatient stay of their surgery.
While potential surprise bills are relatively common, in general, patients with serious or complex conditions may be even more likely to face such charges, depending on the types of services they need and providers they encounter. As this analysis shows, admissions at in-network hospitals for maternity and newborn led to an out-of-network bill about 10% of the time, compared to almost a quarter of admissions involving a heart attack. The higher likelihood of surprise out-of-network medical bills, in turn, increases a patient’s financial exposure. While a person giving birth usually has more time to prepare and presumably plan for in-network provider use than a person having a heart attack would, one in ten maternity-related admissions at in-network hospitals still led to an out-of-network charge. The nature of surprise medical bills is that they cannot be reasonably prevented through planning.
Methods
We analyzed a sample of medical claims obtained from the 2017 IBM Health Analytics MarketScan Commercial Claims and Encounters Database, which contains claims information provided by large employer plans. We only included claims for people under the age of 65. This analysis used claims for almost 19 million people representing about 22% of the 86 million people in the large group market in 2017. Weights were applied to match counts in the Current Population Survey for enrollees at firms of one thousand or more workers by sex, age, state and whether the enrollee was a policyholder or dependent. Weights were trimmed at eight times the interquartile range. Our methods for defining out-of-network claims, in-network facilities and emergency room visits matches the procedure described here. We defined the type of admissions based on the classifications provided in the Marketscan database, similar to the approach used here, which classifies admissions into five categories: surgical; medical; childbirth and newborn; psychological and substance abuse; and, other.
Episodes with heart attacks were defined as outpatient days or inpatient admissions in which enrollees received one of the following icd-10 diagnosis: I2101, I2102, I2109, I2111, I2119, I2121, I2129, I213, I214, I220, I221, I222, I228 or I229.
Women with a mastectomy are defined as women who had claim for a mastectomy or partial mastectomy (CPT codes: 19301 through 19307) and surgical pathology (CPT codes: 88300 to 88309) during 2017. We examined whether these women had any out-of-network claim on any of the outpatient days in which they had a mastectomy or surgical pathology claim. Eighty-one percent of women in this group had a diagnosis of breast cancer (C50). Women who had an ICD-10 diagnosis of F640 or F641 at any point during the year were excluded. Twelve percent of this group had mastectomies on more than one day in the year. Fifty-nine percent of women with a mastectomy had one or two days with a surgical pathology claim in the year, less than one percent had more than six claims in 2017. In-network facilities are defined as either admissions in which a mastectomy was performed and all room and board charges were in network or outpatient days in which a mastectomy was performed and all facility fees were in network.
The Peterson Center on Healthcare and KFF are partnering to monitor how well the U.S. healthcare system is performing in terms of quality and cost.