Each year, health insurers submit rate filings to state regulators outlining their expectations for the coming year and proposing premium changes for Affordable Care Act (ACA)-compliant plans. This analysis examines filings in the small group market, which covers plans offered to small businesses (generally with 50 or fewer employees) through the Small Business Health Options Program (SHOP), state-based exchanges, or directly from insurers.
For 2026, the median proposed premium increase among 318 small group insurers across all 50 states and the District of Columbia is 11%. A more detailed review of filings from 16 states and D.C. shows that insurers cite rising healthcare costs as a primary driver of premium increases. Other contributing factors include higher prescription drug costs and utilization, rising labor expenses, and overall economic inflation. Some insurers also note declining enrollment and worsening risk pool morbidity as factors leading to higher projected costs next year.
How are premiums going to change in 2026?
Insurers in the small group market are proposing a median premium increase of about 11% in 2026
Among the 318 small group market insurers offering ACA-compliant coverage, premium changes for 2026 range from a decrease of -5% to an increase of 32%. The majority of ACA-compliant small group insurers (68% or 216 insurers) are requesting premium increases in the 5% to 15% range, but about 10% (31 insurers) are proposing premium increases of 20% or more. Only 3 insurers have requested rate decreases for the upcoming year. A table in the appendix shows proposed premium increases by state and insurer.
These proposed rates are preliminary and may change; finalized 2026 rate changes are expected to be published in late summer or early fall.
What is driving premium increases?
The remainder of this analysis focuses on a subset of these rate filings (96 insurers across 16 states and D.C.), which were reviewed in more detail to better understand the factors driving premium changes in 2026. Across the 16 states and D.C. reviewed in this section, insurers have a median proposed rate increase of 12%.
Related Content:
Rising healthcare costs
Similar to the individual market, rising healthcare costs are a major driver of proposed premium increases in the small group market for the 2026 plan year. Insurers note that the costs of services such as hospitalizations, physician care, and prescription drugs continue to rise annually, which prompts premium adjustments to keep pace with increased expenditures. For 2026, insurers commonly estimate the underlying increase in the cost of healthcare (medical trend, which is a function of price and utilization) is about 9%.
Inflation and labor shortages
Some insurers cite broader economic factors, including general inflation and labor shortage, as contributing to increased provider reimbursement rates, which in turn place additional financial pressure on insurers and drive up premiums. A handful of insurers have also pointed to increased provider consolidation as a factor reducing market efficiency and raising reimbursement rates.
Tariffs
Some insurers also highlight the potential impact of tariffs, which can raise the cost of pharmaceuticals and medical supplies. When acknowledging the possibility of tariff-driven cost increases, some insurers chose to factor that uncertainty into their rates, while others did not. Of the 96 insurers with filings reviewed in more detail, 23 mentioned the potential impact of tariffs in their rate setting.
GLP-1s and high-cost drugs
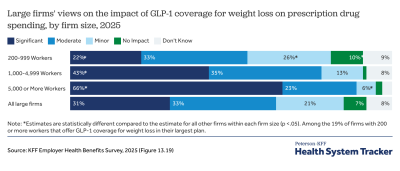
Consistent with premium changes in the individual market, the increasing cost, prevalence, and utilization of GLP-1s and other specialty drugs are frequently mentioned by insurers in justifying proposed rate increases. 27 insurers of the 96 insurer filings reviewed in greater detail mentioned the impact of GLP-1s on premiums. To mitigate their upward pressure on premiums, some insurers have decided to exclude coverage of GLP-1s for weight loss purposes for 2026.
Volatility in the small group market
In addition, several insurers mention volatility in the small group market as a reason for premium changes. Recent volatility in the small group market has been caused by decreases in enrollment for small group plans and a simultaneous increase in relative costs for the remaining risk pool. Insurers point to several pressures destabilizing the ACA small group market through enrollment declines and worsening risk pool health, including competition from relatively lower-cost individual and self-insured options, and state stop-loss rules that can make self-insurance a more attractive alternative for small employers.
“The overall SG ACA market size reduced to just 40.8k members, a reduction of 11.9% over the same period in 2024. We projected that the membership will further decline in 2026 by another 10%.” – Anthem Health Plans of Maine, Inc. (ME)
“IHBC experienced significant losses in membership beginning in 2025 due to various factors such as competitive rate position and overall reduction in the market segment statewide…IHBC estimates that the remaining population to have 1.65% higher expense per member per month than the 2024 base population. Additionally, groups were identified that were in IHBC’s Small Group population in 2024 that have moved to the Large Group market in 2025.” – Independent Health Benefits Corporation (NY)
“Claims from the experience period have been adjusted for anticipated differences in the average morbidity due to anti-selection introduced by the ACA. Groups with better than average experience may not purchase ACA products in 2026 due to the following reasons: (1) Groups may elect to remain on their current (non-ACA compliant) product under the transitional policy guidelines, (2) Groups may elect to move to a self-funded product, (3) Groups may elect to drop Small Group coverage and allow employees to enter the Individual market.” – Physicians Health Plan of Northern Indiana (IN)
On the self-insured side, employers may find coverage less expensive because self-funded plans are not subject to state benefit mandates or premium taxes, and their costs are tied directly to the health of their own workforce. For small employers with healthier-than-average workers, this can be especially attractive. The growing availability of “level-funded” plans, which pair a steady premium structure with substantial reinsurance protection, has further reduced the financial volatility that once deterred smaller firms from self-insuring.
“The proposed rates include a 4% adjustment for ACA market morbidity deterioration. 3% of this is due to continued the migration of groups with lower claims costs to self-funded products. The remaining 1% is due specifically to the change in market size, with an expectation that groups with favorable claims experience will migrate to underwritten Large Group products, resulting in higher market risk for the remaining the Small Group ACA market.” – Rocky Mountain Hospital and Medical Service, Inc. (CO)
Stop-loss insurance also plays a role in this shift; it protects employers by reimbursing them for claims above a certain threshold, effectively limiting their financial exposure. Some insurers in New York cited the state-run Healthy NY Stop-Loss Reimbursement fund, which covers a share of high-cost claims, as lowering or stabilizing premiums. However, recent changes to the program, including increases in the attachment points that determine when reimbursements begin and end, could put upward pressure on premiums. Combined with individual and self-insured alternatives, which rely on private stop-loss coverage and fall outside of state reimbursement programs, these dynamics have contributed to declining enrollment and steady erosion of the ACA small group risk pool.
The relative attractiveness of other markets and the associated decrease in enrollment have caused some insurers to leave the small group market or decrease their availability of plans in a given area. Others have experienced significant financial losses, especially in states with larger proposed premium increases for 2026 such as Ohio (average increase of 16%).
“Due to low enrollment and lack of stability in these pools, we would like to consolidate lines of business under Medical Mutual and, also, offer similar plan options through NWOBA, the Northwest Ohio Business Alliance (a MEWA), whose third-party administrator is Paramount.” – Paramount Insurance Company (OH)
“Claims for this block of business have been very volatile, largely attributed to its low membership volume. In 2024, THP Insurance Company experienced a loss ratio on this business of 116% (calculated as incurred claims divided by earned premium).” – THP Insurance Company (OH)
Methods
Proposed rates were collected from RateReview.Healthcare.gov and the California Department of Managed Care for 318 insurers across 50 states and Washington, D.C. Additionally, 96 insurer actuarial memoranda were collected from state rate review websites (or in the case of Georgia, provided directly by the state regulator) and were reviewed to understand the factors contributing to rate changes. These 96 insurers were from the following markets: Colorado, the District of Columbia, Georgia, Hawaii, Idaho, Indiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, New York, Ohio, Oregon, Rhode Island, Vermont, and Washington. Since rate filings from all insurers in Georgia, Idaho, and Ohio were not publicly available, this analysis only included those filings that were publicly accessible from a portion of insurers in these states. Actuarial memoranda were systematically evaluated for key words related to, but not limited to, medical trend, tariffs, enrollment changes, risk morbidity changes, Individual Coverage Health Reimbursement Arrangements (ICHRAs), specialty medicine, market consolidation, and diabetes or weight loss drugs. Recorded medical trend values are annualized and do not include leveraging.
Appendix
The Peterson Center on Healthcare and KFF are partnering to monitor how well the U.S. healthcare system is performing in terms of quality and cost.