Note: A related chart collection is now updated with more recent data.
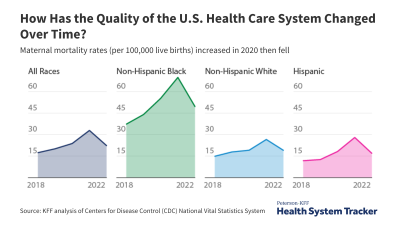
Despite having significantly higher health spending than comparably wealthy and sizable countries, the U.S. lags behind other countries in several measures of health outcomes, with worse life expectancy, mortality, and disease burden rates. Some of this cross-national difference in health outcomes could be due to quality of care provided (a comparative chart collection is available here). Albeit unknown to what degree, some of the difference in costs and outcomes could also be due to societal, economic, and environmental factors that influence health but are in some respects outside the control of the health system. Our latest chart collection explores international comparisons of some of these factors, broadly referred to as social determinants.
The U.S. spends less than other countries on non-health social services, but much more on health Share on XAlthough varying models exist, consideration of social determinants of health generally includes: individual and community behaviors, economic circumstances, and environmental factors. Our analysis does not intend to be a comprehensive look at all factors that could be considered social determinants – nor does it aim to isolate a set of health determinants outside the realm of the health system. It aims instead to gather data we do have about some of the better-understood factors that may influence health. These data are limited, and won’t allow us to pinpoint, for instance, the effect of income on diabetes outcomes. Rather, these data can give us a sense of whether the U.S. has higher rates of external factors that might negatively influence health outcomes or lead to higher spending relative to similarly sizable and wealthy OECD countries.
The complex nature of social determinants makes it difficult for researchers to estimate the relative contribution to health. Racial health inequalities, for example, can coincide with other socioeconomic factors that affect health, such as income and education. Additionally, the relationship between social circumstances and health is not always unidirectional. For example, having a lower income can lead to healthcare access barriers and difficulty living a healthy lifestyle, while in turn, poor health can lead to an inability to work, and thus lower income. And while cross-national assessments of social determinants of health are a useful compass, comparisons are complicated by differences in measurement, as well as national demographics (including race and age).
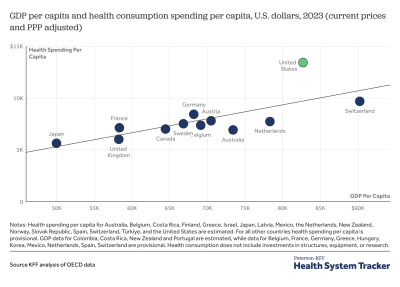
The U.S. is an outlier for health spending, but when combined with other social services, spending is similar to other countries
While the U.S. is an outlier for health spending, its spending looks more similar to that of other countries when health spending is combined with spending on other social services (such as cash assistance and other support for the elderly, poor, unemployed, and other disadvantaged or vulnerable populations). This is because the U.S. spends less than other countries on non-health social services, although such programs could indirectly improve health.
Related Content:
How the U.S. Compares on a Variety of Social Determinants
Although the aging population in the U.S. explains some of the growth in health spending, compared to other wealthy countries, the U.S. has a younger average age (38 years old vs. 42 years old) and smaller percent of the population over the age of 65 (14% vs. 18% on average).
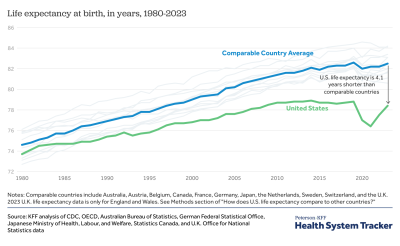
Life expectancy at birth in the U.S is lower than comparably wealthy and sizable OECD countries. In 2013, the U.S. life expectancy was just under 79 years, compared to an average of just under 82 years for comparable OECD countries. Racial disparities may contribute to the United States’ relatively low life expectancy, but it is unclear how much or in what way. Despite improvement in the racial gap in life expectancy in recent years, Black Americans continue to have shorter life expectancies than those who are White or Hispanic. Meanwhile, women in the U.S. have seen slower improvement in life expectancy than women in other countries, gaining four years of life expectancy at birth since 1980, compared to six years in comparable countries on average.
A large body of research has examined the ways in which income can significantly influence health outcomes. People with a lower income are less likely than those with higher incomes to report being in good health, and there is a growing disparity in the life expectancies of low and high income Americans. While income is also correlated with behavioral factors that can influence health, recent research has found that these factors only explain some of the difference in outcomes between low and high income people.
The U.S. has a higher degree of income inequality than comparably wealthy countries
The U.S. has a higher degree of income inequality than any comparably wealthy and sizable country. In 2012, the most recent year where data are available for the majority of comparable countries, the U.S. had a larger-than-average wage gap between males and females. Disparities can also be found across smaller geographies; the Robert Wood Johnson Foundation’s County Health Rankings reports have found that the least healthy American counties also tend to have higher degrees of income inequality, along with higher rates of unemployment and lower graduation rates.
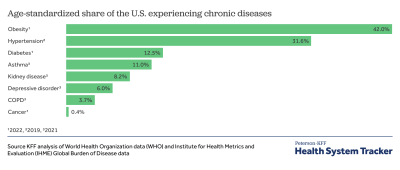
The U.S. has the highest environmental burden of disease of comparably high-income countries Share on XData on behavior and lifestyle-related social determinants of health, such as diet and exercise, show that the U.S. has long had a higher per capita fat and caloric intake than comparable countries, as well the highest prevalence of obesity (35.3% vs 21.2% average across comparable countries) and insufficient physical activity among adults (32.4% vs 26.4%). Despite smoking fewer cigarettes per capita and consuming less alcohol in terms of liters per capita, the U.S. has higher-than-average disease burden from lung cancer and alcohol abuse. Research has shown that in countries where alcohol consumption is more restricted and less frequently integrated into meals and other daily activities, such as the U.S., Canada, and much of Scandinavia, more people tend to abstain from drinking, but those who drink do so more heavily and are more likely to become intoxicated.
External causes (such as accidents, suicides, and violence) are the fourth leading cause of death in the U.S., and are more common than in comparable countries. According to data from the Centers for Disease Control and Prevention, unintentional poisonings (often due to prescription drug overdose) are the leading cause of accidental death in the United States. The U.S. had a higher than average mortality rate from accidental poisoning in 2000, but over time, the U.S. has become an outlier, now with far higher death rates from accidental poisoning than any comparable country.
In addition to accidental death, violence is another type of death due to external causes. In the U.S., 206 years of life per 100,000 people are lost to disability and premature death as a result of assault by firearm – almost 16 times the comparable country average of 13.1 years of life per 100,000 people.
The U.S. also has the highest environmental burden of disease of comparably high-income countries. The World Health Organization quantified the effect of environmental factors, such as pollution, occupational risks, agricultural methods, climate change, and food contamination on disease burden (measured in Disability Adjusted Life Years, or DALYs. Taken together, these factors present a higher burden of disease in the U.S. (1,861 DALYs per 100,000 capita) than in comparable countries, whose average environmental burden of diseases is 1,590 DALYs per 100,000 capita.
Discussion
There are more gaps in our understanding of social determinants than there are answers, and it is important to keep in mind that cross-national comparisons of these factors would not necessarily parallel differences in cross-national health outcomes. Consider alcohol intake, for example. Even though the U.S. has lower per capita alcohol consumption, data on disease and death with known links to alcohol use suggest that it presents more of a burden on health outcomes in the U.S. than in comparable countries. Alcohol intake varies by drink strength, type, and frequency of consumption, and research indicates that differing drink cultures may result in varied health outcomes. Cross-national comparison of these types of indicators should be used with care, as cultural and market-based differences are bound to shape lifestyle and behavioral factors in ways that we cannot reliably measure.
Literature does indicate, however, that the U.S. spends disproportionately more on healthcare than on other social services, compared to other Western countries. The ACA has stimulated considerable interest in the significance of broader determinants of health, due to its focus on preventative health, primary and integrated care, community needs, and new forms of health care delivery and payment. Yet there are limitations to developing policies based on social determinants. The mechanisms by which determinants shape health outcomes are not always clear. Also, behavioral change can be difficult to shape through policy, which we see exemplified by efforts to reduce sugar consumption (and thus the prevalence of obesity and diabetes) through legislation either limiting or taxing sales of soda and other sugary drinks. New York City’s proposal to limit the serving size of sugary drinks was ultimately rejected, and although legislation taxing high-sugar drinks passed recently in Berkeley, CA and the Navajo Nation, the impact of such policies on health outcomes and related behaviors is again difficult to parse from other factors.
Social circumstances and unhealthy behaviors no doubt influence health outcomes, but it is up for debate how much the health system itself can address these factors. Some providers are quite reasonably concerned about being held accountable for patient circumstances that are largely outside of providers’ control. Nevertheless, providers can play a role in connecting patients to other services and guiding them toward healthy behaviors. Some academic medical centers, for example, are beginning to shift away from a sole focus on individual patient care and toward a broader goal of improving population health. In its recent report on health quality measurement, the Institute of Medicine similarly looks beyond what might be considered the healthcare system and includes measures that address societal factors, such as rates of high school graduation, addiction, health literacy, and community support. While addressing social circumstance is not the primary responsibility of the health system, and improving health is likewise not the primary responsibility of social service programs, finding ways to coordinate the two types of services may improve both health and wellbeing, and potentially do so at a lower cost.
The Peterson Center on Healthcare and KFF are partnering to monitor how well the U.S. healthcare system is performing in terms of quality and cost.